
Pacific scientists work to combat malaria
Scientists in the region are setting their sights on the parasite Plasmodium Vivax as the key to realising the Pacific's aim to eradicate malaria.
Transcript
Scientists in the region are setting their sights on the parasite Plasmodium Vivax as the key to realising the Pacific's aim to eradicate Malaria.
Recent research conducted by the Walter and Eliza Hall Institute in Melanesia has revealed that Plasmodium Falciparum the other malarial parasite common in the Pacific has been all but wiped out in the region.
But Plasmodium Vivax remains prevalent because of its ability to lie dormant in the liver for up to four years before reinfecting its host and starting another wave of transmission to other human beings via mosquitoes.
The institute's head of Population Health and Immunity Ivo Mueller spoke with Koroi Hawkins about the problem and a possible solution.

Dr Leanne Robinson (far right) with patient Jonathan (far left), who is being tested for malaria by Nursing Officer Kay Kose (second from left) and microscopist Barbara Sambre (second from right) in Papua New Guinea. Photo: Mayeta Clark/Walter and Eliza Hall Institute
IVO MUELLER: So over the last 10 or 15 years we have seen a very significant reduction of malaria in the Pacific and particularly in Vanuatu, Solomon Islands and more recently in Papua New Guinea. But with this reduction we have also seen a shift from a lot of falcipural malaria to much more vivax malaria and in countries like Vanuatu and Solomons the vast majority of malaria now is vivax malaria. So if these countries want to continue along this track and actually eliminate malaria so get rid of it completely plasmodium vivax turns out to be the hard last part that needs to be solved. And what we have shown in our research is that one of the main reasons why vivax is so hard to get rid of is that it can survive in the liver in a dormant stage that can remain for months even three or four years. Later it can reemerge from the liver and cause a new infection and then transmit again to the mosquito and then on to the next person. And we shown in a study in PNG that these relapsing infections account for 80 percent of four out of five infections that children in Papua New Guinea have are not caused by a new mosquito bite but from a dormant stage that comes back out from the liver. So if we want to make rapid progress towards elimination we really have to deal with these dormant stages.
KOROI HAWKINS: Now there is an issue with this in terms of a real world application of this idea in that the treatment for such liver born malaria parasites is actually quite long isn't it?
IM: The problem is that the only drug that we currently have that is licensed for this use which is a drug called primaquin it is a 60 year old drug. It has to be given to 7 to 14 days we usually use a 14 day course in the Pacific. And it is not only that it is very difficult to get people to take it for 14 days, but also that in some people that have an enzyme deficiency called G6pd deficiency we actually shouldn't be treating people because the drug can lead to haemolysis and therefore lead to people becoming anemic if they take that drug. Not necessarily very sever anemia but people can become anemic. So because of this problem of compliance and problem of safety in G6pd deficient people, we, the countries have not very thoroughly implemented treatment of vivax with primaquin.
KH: And are you suggesting any alternative are you suggesting a solution to this issue?
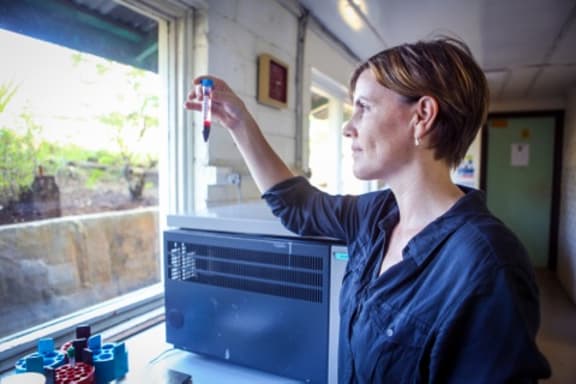
Dr Leanne Robinson with a blood sample in the Papua New Guinea Institute of Medical Research Lab. Photo: Mayeta Clark/Walter and Eliza Hall Institute
IM: Our modelling the mathematical modelling that we have done shows that really the most effective way of dealing with this is to do mass drug administration, so really go out and treat entire populations. Give primaquin and other malaria drugs to all people in a community and that is the way how we could relatively quickly eliminate transmission. And this actually has been done on a small island in Vanuatu where this has been shown about 10 or 15 years ago that this actually can eliminate malaria completely from these small islands. So it is feasible it is doable. But the challenge is that for instance again in the Solomon Islands if we go and we treat only the people who we know have the infection in their blood we probably miss about two thirds of people that have parasites in the liver that need to be treated. On the other hand only about 70 percent, 30 percent of people actually do have any infection over the course of a year. So if we treat the entire population we will treat 70 percent of people with a drug that they don't need. And so we have a, we need to find ways of bridging that gap between not treating two thirds of the people we need if we only do people with infections we can diagnose. Or treating 70 percent of people that don't need any drugs. So what we are trying to do hear at the Walter and Eliza Hall Institute to address this is that we are, have received funding from the Japanese government as well as the Australian government. To develop a diagnostic test that could help us detect the people that are likely to have these liver stages. And if the development of this test works and it performs the way we think then we could target people directly with treatment and people we know have these liver stages.
KH: So what is the timeline on that research and on developing that test?
IM: We hope to have a pilot test within the next 18 months?
KH: And that will be rolled out, will you be testing it in Australia or will you be taking it out into the Pacific?
IM: The development of the test for a pilot test is the development happens here in Australia as well as in Japan and then once we have a pilot test it will take a little bit longer to make that test available for actually malaria control programs. But we will be trialling it probably first in Papua New Guinea probably hopefully in 2018, 2019 where we want to do some pilot implementation trials to see whether that test really does what we hope it will.

