
Increasing access to the pill comes with risks, especially when it’s prescribed for reasons other than birth control.
Photo: Illustration: Tiggy Cameron
Tiny, sugar-coated pills encased in colourful blister packs symbolise a sexual revolution that occurred well before most current pill-taking women were born.
The oral contraceptive pill has revolutionised women’s health and reproductive rights since it was first introduced in the 1960s, but many of its side-effects have seen little improvement beyond its inception.
Depression, blood clotting, increased risk of breast and cervical cancer and stroke are just some of the side-effects recognised as “normal” by the medical profession, and while its contraceptive benefits are undeniable, the pill is no longer prescribed for birth control alone.
More than 200,000 women in Aotearoa currently take the pill, prescribed for a myriad of women’s health issues — from acne to period pain. The Ministry of Health does not collect information as to why the pill is prescribed, though a US report estimates that 58 percent of women taking the pill in the US do so for non-contraceptive reasons.
Medsafe’s recent reclassification of the oral contraceptive pill to a “restricted” medicine will allow women to access repeat prescriptions from a pharmacist, provided they are aged 16 and over and have been prescribed the pill by a doctor in the previous three years.
While the move to increase access to oral contraceptives has been welcomed by most, there is concern among women that the pill has become a quick fix for a multitude of health issues.
***
“It’s not really a contraceptive pill anymore, it’s a pill for the ‘problems’ associated with being a woman,” says Ella**, 27, a lawyer in Dunedin.
Ella stopped taking her combined oral contraceptive pill last year after reading about its link to mental illness. She had been feeling out of sorts for a while and decided it was time to give her body a break.
She was surprised how she began to feel after discarding the pills that had sat on her nightstand for more than a decade.
“It was like this fog lifted and I became a totally different person. I was happier all of a sudden and had a way better outlook on things,” says Ella, who was prescribed the pill for period pain at age 15 and had been taking it ever since.
“But I felt kind of cheated and like I had wasted all these years of my life just feeling sort of blah.”
She started talking to friends, an aunt, colleagues and her hairdresser, all of whom had similar experiences coming off the pill.
They were honestly like sales people. I told them what had happened and asked about alternatives but they just brushed it off. They didn’t want to know.
“It was crazy that all these women had these bad side-effects, some a lot worse than me, but whenever you go to the doctor they essentially throw the pill at you and send you on your way.”
Earlier this year, Ella’s skin broke out. She visited her GP who told her the best option was to go back on the pill. Determined not to, she tried another doctor who told her the same thing.
“They were honestly like sales people. I told them what had happened and asked about alternatives but they just brushed it off. They didn’t want to know.”
On a friend’s recommendation, she visited a natural practitioner who pinpointed the cause of her acne to a stressful new job and a resulting change in diet, and with a few lifestyle changes her skin has since cleared up. She has also started using a natural contraception method and says she is starting to feel “like a real woman” again.
“A doctor should have asked me about that stuff instead of just sticking me back on the pill,” she says.
“Our generation is so conscious about things being natural, you know, we take our own bags to the supermarket, we spend all our money on organic skincare, yet here we are pumping these shitty, artificial hormones through our bloodstream when there are much better alternatives that we’re not told about."
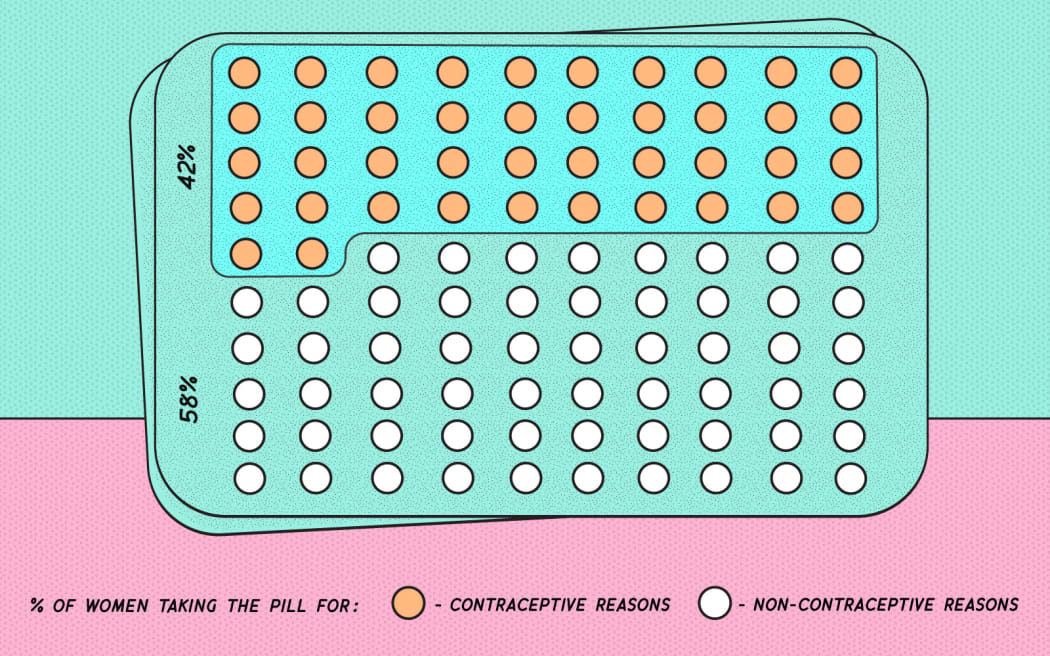
*According to research by the Guttmacher Institute. Photo: Illustration: Tiggy Cameron
Ella’s story is echoed by women the world over, for whom the pill has become a widely-prescribed cure-all with harmful side effects and seemingly few alternatives.
Dr Judith***, a GP with a special interest in women’s health, says the pill is “generally a safe medication” but it does have risk factors, and every patient assessed needs a risk profile which considers whether they are taking other medications and family history of associated conditions.
There are a lot of variables that you have to take into account when renewing a prescription, and you need a lot of knowledge on the subject.
She says repeat appointments for the pill usually take 10-15 minutes and is concerned that pharmacists may not have time to ensure adequate patient care.
“There are a lot of variables that you have to take into account when renewing a prescription, and you need a lot of knowledge on the subject. I am concerned that knowledge is not going to be learnt in a couple of workshops.”
***
“I wish I’d never met Estelle,” says Lucy, 26, a music teacher in Wellington who stopped taking her oral contraceptive pill, Estelle-35ED, earlier this year.
“I’m only just getting to know my body and my cycle and learning that what I thought was abnormal is in fact just what my body feels like when I have my period.”
Lucy was prescribed the pill at age 15 for heavy and often painful periods, and while her cycle soon became more manageable, she describes her time on the pill as a “confusing decade”.
My acne was moderate at the time and I remember thinking it seemed pretty full-on to be taking both medications but, hey, anything for clear skin right?
“At no point was it ever discussed with me or seemingly considered that my contraceptive pill may or may not have played a part in an ongoing battle with my mental health,” says Lucy, who was prescribed Escitalopram for depression and anxiety at age 21.
She continued taking the pill when she became sexually active, but when she started dating women in her early twenties, Lucy decided Estelle was probably no longer useful. However, her doctor recommended she keep taking the pill alongside her acne medication, Isotane, to keep her skin clear.
“My acne was moderate at the time and I remember thinking it seemed pretty full-on to be taking both medications but, hey, anything for clear skin right?”
Since coming off the pill, Lucy’s depression has subsided, but she still struggles with anxiety. She says her experience of doctors’ willingness to prescribe the pill for non-contraceptive reasons shows an “apathetic approach” to women’s health.
“The fact that I was on the pill and there were no dicks in my bed is kind of like case in point, right?”
***
Anna, 26, a producer based in Auckland has been taking the pill since she was 18, when it was prescribed to her for endometriosis, which caused her to suffer from non-stop periods and crippling stomach cramps.
She says the pill has been a “lifesaver” but is worried about its long-term health effects and would like her doctor to discuss safer options with her.
“I would be interested in alternative options if they were healthier and took away the risks that come with the pill. I’m definitely a believer of avoiding putting those sorts of things in your body if you don’t need them.”
Anna has changed pills a number of times due to what she describes as “pill-induced depression”.
“I had a crazy time in second year at university when I thought I was really depressed and didn’t know why. I ended up getting counseling, but then I randomly changed pills and felt like the weight of the world had been lifted off my shoulders.
“I definitely think doctors need to be way more careful with the pill and check up on things like mental health more. I had no idea it could be the pill that was making me feel that way.”
***
It’s not an “absolute prerequisite” to question patients about their mental health during a consultation for the pill, says Dr Judith.
“But if a patient is taking anti-depressants or has previously been admitted to hospital for mental health concerns I would go into it more deeply,” she says.
While increased access to oral contraceptives is great for women’s health in some respects, Dr Judith does have her concerns about the reclassification.
For some women, the cost of accessing the pill from a pharmacy will actually be higher.
For women under 22, a consultation appointment at Family Planning clinics is free, with a $5 prescription charge for a six-month supply. According to Green Cross Health, which represents Unichem and Life pharmacies, a three-month supply from pharmacies will cost approximately $45.
Being able to pick up the pill over the pharmacy counter is no doubt convenient for those who can afford it, but there is concern that the reclassification may have missed the mark for those most at risk of unplanned pregnancies.
“I understand that access can be difficult with doctors, but I do question the motivation behind this [reclassification]. My feeling is that it’s perhaps a drive to make more money rather than to improve women’s accessibility to the medicine,” says Dr Judith.
When the pill is taken for contraceptive reasons, the risks are balanced with preventing pregnancy, says Dr Judith, but when it is prescribed for other issues, there is more risk involved. For conditions like acne, she says it’s better to start with less harmful options such as topical treatments, especially for younger women.
“The pill will probably improve the pain or the acne, but that doesn’t give you the answer to why it’s occurring in the first place and it’s important to ask why - to get to the bottom of things before just sticking [women] on the pill.
“Doctors must look at the causes rather than just prescribe treatment. There’s not always a lot of choice, but it’s definitely good to start with the lesser options. That’s how medicine should be.
“Don’t just bang them on the pill.”
***
The notion that doctors are overprescribing the oral contraceptive pill is “completely incorrect and inappropriate”, says Dr Tim Malloy, president of the Royal New Zealand College of General Practitioners — the professional body for practising GPs.
“I don’t know who would do that. A lot of patients just don’t understand the thinking behind an outcome.”
However, Dr Malloy says when a woman is prescribed the pill for non-contraceptive reasons, they may only need to take the medication for a short period of time and the fact that young women are staying on the pill for many years is “concerning” and can have long-term health implications.
I don’t know who would do that. A lot of patients just don’t understand the thinking behind an outcome.
He says while the safety provisions as part of the reclassification have come a significant way to addressing concerns GPs have about safety, pharmacists are not trained to the extent doctors are on how to use the pill appropriately. He is also concerned that the high cost of repeat prescriptions from a pharmacy will increase women’s health inequity.
The New Zealand Medical Association also has a number of concerns about the reclassification, says its chair, Dr Stephen Child. He is worried it will remove the opportunity for women to have an interaction with their GP on issues relating to sexual health, undermining the “therapeutic relationship” between doctor and patient.
Dr Child says the NZMA is also concerned that the proposal does not actively encourage the uptake of long-acting reversible contraception (such as IUDs) which “has been shown to be more effective in practice than contraceptive pill use.”
***
Eilidh, 25, describes herself as a “huge proponent” of IUDs, after recently having her second intrauterine device inserted.
She was prescribed the pill for acne at age 15 but was taken off it at age 19 to reduce her risk of stroke after she started having migraines. She tried a number of other contraceptives, including an implant and the minipill, and finally settled on the Mirena IUD, which is subsidised in the UK (where she now lives).
Eilidh says she is surprised IUDs are not as commonly prescribed in New Zealand for both contraceptive and non-contraceptive reasons.
“The nurses who I spoke to when I had my IUD changed [here] said they generally suggest [them] as the best form of long-term contraception for women of all ages and generally stay away from prescribing the pill now.”
When Eilidh was first prescribed the pill, she says there was no discussion of other possible ways to treat her acne.
“I appreciate the pill is prescribed for more than just contraception, but I think healthcare professionals need to be much more open to alternative methods of treating acne and period pain than just immediately prescribing the pill, especially to teenage girls.”
***
Maia*, 23, a reporter based in Auckland, started taking the pill at age 15 for endometriosis. After 10 weeks she experienced what she describes as “weird, warm, sharp pains” in her right leg and was taken off the pill by her doctor due to suspected blot clotting.
Because she is unable to take the pill, Maia has explored a range of other contraceptive methods, and is concerned that medical professionals are quick to prescribe the pill without first discussing other localised contraceptive options, such as IUDs.
“Women should have a really good knowledge of all the products available to them, for contraceptive [reasons] or otherwise, but many do not.”
“All medications have side-effects and people, of course, need to be cautious of that, but so many women, young girls especially, go to their doctor or family planning clinic and ask for the pill because it’s the only form of contraception they’ve heard of…”
Photo: Illustration: Tiggy Cameron
Countries that offer birth control pills over the counter include China, South Africa and India. But in Australia, the UK and most states of the US, a doctor’s prescription is still required.
The reclassification will come into effect once it is published in the New Zealand Gazette, which was expected at the end of February, and Medsafe manager Chris James says the availability of oral contraceptives from a pharmacy will only commence once pharmacists have been deemed appropriately trained.
**Some women’s names have been changed due to the personal nature of the information disclosed.
***Dr Judith did not wish to disclose her full name in order to avoid backlash from her employer and/or medical colleagues.

